Introduction
Higher education in nursing started in Finland at the beginning of the 1990s. The establishment of tertiary education in nursing was part of an academic drift towards developing the formerly non- university-based, vocationally oriented courses into an internationally more comparable educational model and to develop a nursing education that can serve the changing needs of the rapidly developing world of work. (Pratt 1997; compare Ahola 2006) The education is organised in Universities of Applied Sciences, which have since 2002 also offered practice-oriented Master’s level degree studies. The current Bachelor-level education lasts for 3.5 years and the matriculation examination or vocational education is required from all applicants. (Statute 351 / 2003; 351 / 2003)
The main aim in developing nursing education into a higher educational programme was to enable students to obtain a comprehensive picture of the role of nursing in the Finnish health care. This meant expanding the view of nursing not only in this society but also internationally. It was considered important to enable nurses to acquire a higher level of training in the field of nursing. Previously, vocational nursing education had provided the knowledge and skills for nursing practice, and one aim of higher education in nursing was to develop inquiring minds in the students, in addition to transferring knowledge and skills. The overall aim was to educate a new kind of personnel that can promote innovative changes in the profession (Pratt 1997).
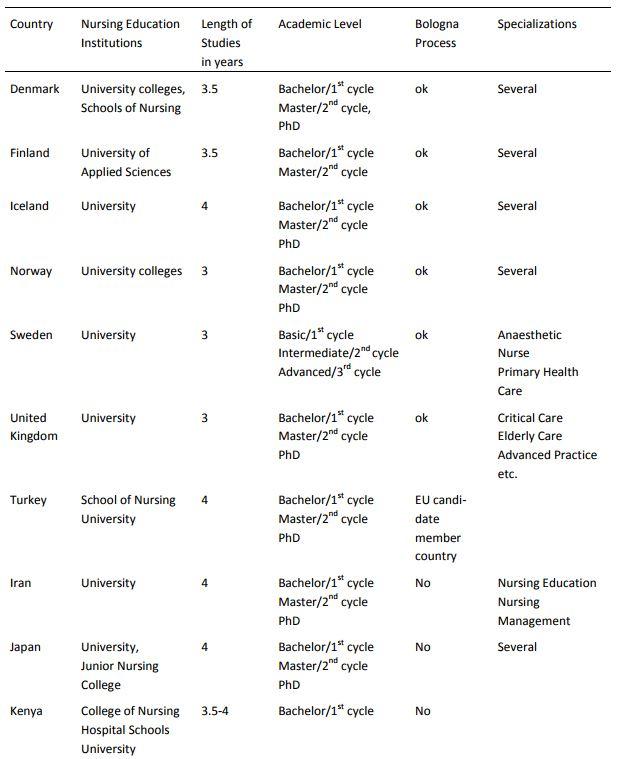
At the end of the 2000s, higher education in nursing in Finland has become well established. This reform in Finnish nursing education has taken into account the Bologna Process, which aimed to create by 2010 a European Higher Education Area where students can choose from a wide and transparent range of high quality courses and benefit from recognition and accreditation procedures. The Bologna Declaration of June 1999 put into motion a series of reforms to make higher education in Europe more compatible, more comparable and more competitive. As a result, nursing students can participate in student exchange programs and nurses can work in the other signatory countries. This kind of nursing education is also available outside Europe: for example, Turkey strives to develop its nursing education in line with the Bologna Declaration. Some central features of nursing education in selected countries are presented in Table 1, based on articles in international journals of nursing (Bahcecik & Alpar 2009; Davies 2008; Khomeiran & Deans 2007; Kyrkjebo et al. 2002; Svavarsdottir 2008; Turale et al. 2008).
Nursing studies at the academic level first commenced in the University of Kuopio in 1979 in the administrative training program. Studies in nursing administration, nurse teacher training and nursing science were organized in the universities in full by 1996. To be able to apply for these programmes, the applicants had to have a nurse specialist qualification. In several countries Master’s level education can be completed either with or without honours, i.e. with emphasis on research studies or with specialization. However, Finnish nurses specialize already during their studies at Bachelor-level, while academic research studies are completed during Master’s degree studies. The development of Master’s level nursing studies has strengthened the research orientation of Finnish nurses. (Kuuppelomäki & Tuomi 2005).
The aim of the reform in nursing education in Finland was to produce nurses who are able to take more responsibility in nursing and can become equal members of multi-professional teams in health care. Before higher education in nursing was established, there had been a national curriculum for nurse education. After the reform in the 1990`s every school of nursing at the Universities of Applied Sciences had to create an individual nursing curriculum for their institution. Besides the content of the curriculum, nursing schools also defined the learning approach they were planning to use. Mainly the schools chose to adopt the ideas of the cognitive view of learning, and therefore underlined the importance of supporting the idea of students’ self-directed learning. (Ponkala 2001; Perälä & Ponkala 1999)
The aim of this article is to describe how the learning approach of nursing students has changed since 1990’s. The data were collected from Universities of Applied Sciences in different parts of Finland during 1996-1997 and 2006-2007. The paper reveals the changes that occurred, and offers some similarities and differences between them.
The approaches to learning nursing
The focus in the training type curriculum had been in clinical skills and nursing care of patients mainly in hospitals (Roxburgh et al 2008). The learning approach used in this kind of nursing curriculum until the 1980s can be described as a didactic learning process. This approach to teaching and learning has also been referred to as the behaviouristic paradigm (Romyn 2001). In this approach, the nursing teacher is considered to be in possession of the necessary knowledge and also knows how to transfer it: in other words, she knows how to teach students. Students are expected to be able to apply this knowledge, first during their laboratory studies, and then in their nursing practice in patient care. Similar features of the learning process have also been described in pedagogy (Knowles 1980) and single loop learning process (Greenwood 1998).
The early 1980s was a turning point in the views of learning in nursing curricula. Student-centered views of learning began to gain more significance in nursing curricula. In Finland, this shift started in the mid-1980s, following the ideas of Marton and Säljö (1976). This learning approach can be associated with constructivism and meaningful learning, which are related to cognitive psychology and the humanistic-psychological model of learning (Apodaca & Grad 2005; Ausubel 1978). The approach emphasised students’ abilities to be active learners who improve and modify the structure of their knowledge. Earlier experiences, knowledge and attitudes influenced the students’ learning process. The teachers role is to support the learner to find information and insight, and to identify learning and work-related problems.
As mentioned earlier, in the 1990’s the idea of students’ self-directed learning was emphasised in the nursing curricula. Self-directed learning is possible when the methods of learning support the students’ own possibilities to plan, carry out and evaluate their learning process (Levett-Jones 2005). Methods such as learning diaries (Blake 2005) and portfolios (Williams & Jordan 2007) have been tested to enhance critical thinking, meaningful and active learning and reflective practice. Portfolios focus especially on supporting students in managing change efficiently. They also help them in terms of self-directed learning to find ways which will assist them in enhancing the quality of their learning activities. Actually, both concept mapping (Hay 2008; Abel 2006; Hsu 2004) and portfolios (Bashook et al. 2008) have been suggested to be very useful in e-learning, too. The self-directed learning approach has changed the role of the teacher, as well. Teachers are seen as facilitators (Badeau 2010, Williams 2004), defined in terms of genuine mutual respect, a partnership in learning, a dynamic, goal-oriented process, and critical reflections between the facilitator and the student. This conception is also connected with the humanistic paradigm in nursing education (Gillespie 2005).
Besides the view of self-directed learning, the co-operational learning became more popular also in the nursing curricula during the 2000’s. Several situated learning theories (Lave & Wenger 1991) and work-based learning (Guile & Griffits 2001) approaches describe the possibilities of learning from one another, and of learning in teams, in terms of democratic dialogues and co-operational meetings. Moreover, the situated learning theory assumes that knowledge is embedded within the context in which it is used and cannot be separated from the activity, context, and culture of that situation (Lave & Wenger 1991; Engeström 2001). Co-operative learning and situated learning have been highlighted as necessary for learning the co-operational methods needed to function as a member of a multi-professional team working in complex situations in health care (Tynjälä 2008). In co-operative learning the ownership of teaching and learning is shared by the students.
The aim of the study and study questions
The aim of the study was to describe how the learning approach of nursing students in Finland has changed since 1990’s . This study set out to answer the following questions from nursing students’ point of view:
i) to what extent did Finnish nursing students demonstrate and express the features of assisting, self-directive and co-operational actors in 1996-1997 and in 2006-2007, as their approach to learning nursing?
ii) what differences are there in nursing students’ approaches to learning nursing between the years 1996-1997 and 2006-2007?
iii) to what extent do the background variables (age, sex, professional or lay experience in nursing) explain the differences in students’ approach to learning nursing between 1996- 1997 and 2006-2007?
Methods
Sample and data collection
The data was gathered during 1997 and in 2006-2007 in nursing schools in Universities of Applied Sciences in northern, western, central, eastern and southern Finland in order to get geographically and regionally relevant information.
The amount of nursing schools in the Finnish Universities of Applied Sciences was 24 in 1997, 23 in 2006 and 22 in 2007. The total amount of nursing students in Finland was 5,589 students in 1997, 6,891 students in 2006 and 7,545 students in 2007. Four schools were chosen into the sample in 1996-1997 and six schools in 2006-2007. Three of the schools were the same in both phases of the data collection. The number of nursing students in those sample schools was 712 students in 1997, 2,056 students in 2006 and 2,141 students in 2007. (Finnish Ministry of Culture and Education, online statistics 14 April 2011)
The nursing students (N=1,086) voluntarily answered the questionnaire: 426 in 1997 and 660 in 2006-2007. The response rate in 2006-2007 was 76.4%. In 1997 the researcher administered the data collection at schools. In 2006-2007 the questionnaire (N=864) was delivered to students by the research assistants. The questionnaire was given to all nursing students, who were having their theoretical study period during the data collection (simple random sampling). In 1997 37.5% of the respondents were first year students and 40.1% final year students. Information was missing from 22.5% of the respondents. In 2006-2007, 57.4% of the respondents were first year and 42.6% last year students.
The questionnaire contained questions concerning background factors and 26 Likert-type statements. The following background factors were elicited: sex, age, any children, pre-educational caring experiences and intentions to leave nursing. The statements were designed on the basis of a literature review. The tool consists of three sub-scales measuring nursing students’ approach to learning nursing; the assisting, self-directive and co-operative actor approach. Each sub-scale includes statements measuring the relationship between nursing student and nurse teacher/supervisor, the relationships with peers while learning nursing, and nursing students’ views of learning and of responsibility in the field of nursing
The student with assisting actor approach needs the teacher’s and supervisor’s support, and the encouragement of peers. She is willing to work with an experienced nurse and is able to work as a reliable member of a nursing group. However, she is not willing to take personal responsibility in patient care.
A self-directive actor sees teachers, supervisors and other experts primarily as facilitators who share information with her. Such students want to learn to make decisions independently. They want to develop their individual structure of knowledge continually and develop an inquiring mind towards their work and working environment. They want to learn to take responsibility in their given field.
The co-operational actor wants to test her knowledge, ideas and practices together with peers and a multi-professional team in practical situations during her education. For these students, learning is not an individual but a shared experience. It is possible to create new practices and to evaluate them while learning nursing and developing patient care in health care practice. Co-operational actors are willing to take responsibility as individuals and as members of a multi-professional team.
Ethical questions
In Finland, the permission of the Ethical Committee is not required if the research does not deal with patients or other vulnerable groups. After gaining approval for the research from the institutions (today they are called Universities of Applied Sciences), the researchers contacted nursing teachers. The teachers who agreed to participate asked the students to take part in the study and then organized the data collection. Completing the questionnaire was voluntary and the students answered anonymously.
Data analysis
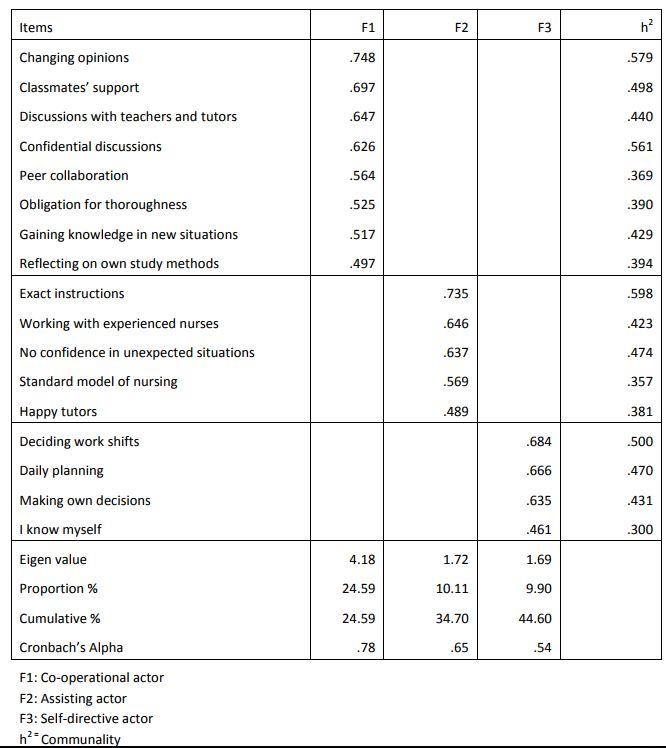
The data were analysed using SPSS for Windows 15.1. Factor analysis was used to compress information into smaller units. The principal component method and Varimax rotation were used in factor analysis. The criteria for separating the variables for factor analysis were the following: sufficiently high loading of items on the factors (≥ .40), high communality values (≥ .30) and as clear a solution as possible. Three factors emerged: co-operational actor, assisting actor, and self-directive actor (Table 2). The sum scores were calculated for each factor. The internal consistency of the sum variables was tested using Cronbach’s alpha coefficient. The Mann-Whitney U-test and Chi-Square test were used for testing the change between the 1990s and the 2000s. The Chi-Square test was used to test the similarities in the demographics. There were only slight differences (max. 10 %) in the demographics between the two time periods of data collection.
Reliability and validity of the measurement tool
The validity and reliability of the measurement tool were tested before use in this study by panel evaluation and subsequently by using psychometric measurements. An expert panel assessed the validity and reliability in terms of readability, homogeneity and content validity using a paper and pencil test. The panel members (Finnish nursing students) assessed all items in terms of clarity and content validity. The agreement on homogeneity with all items was over .60.
Actually, the sumscores used were on ordinal data. However, when using this kind of scale the sumscores can be handled as continuing variables. The Cronbach alpha coefficient was .759 on the whole scale, and validity was measured using explorative factor analysis, which supported the three- factor solution (Nunnally & Bernstein 1994) (Table 2). The value of alphas in the subscales varied from 0.78 to 0.54, which can be seen rather low. However, it is notable that the value of alpha varies according to the number of variables in the measurement tool and subscales, i.e., the more variables, the higher the alpha (Carmenis & Zeller 1979).
Results
Students’ background factors
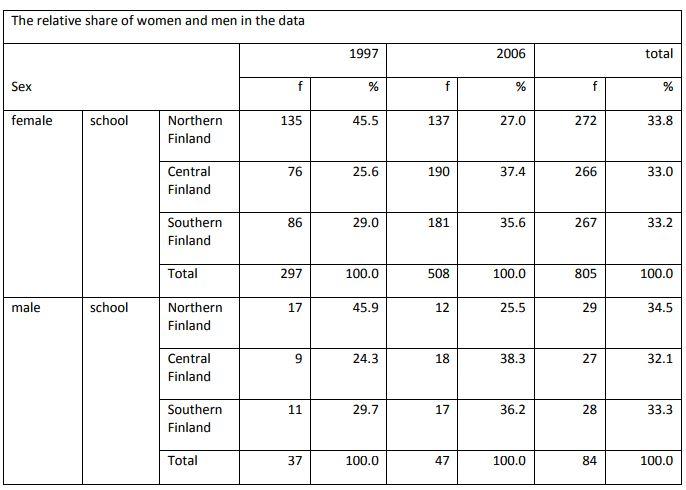
Most of the participating students were females in both the 1990s (90.4%) and the 2000s (92.4%). In fact, the distribution between the sexes was about the same as it is in nursing in general in Finland (Finnish Ministry of Culture and Education, online statistics 14 April 2011). Moreover, there was not a big difference concerning the age distribution, either: more than half of the participants were in the youngest age group. Furthermore, the nursing students of the 2000s had more professional nursing experience than those of the 1990s. In effect this meant that the nursing students of the 2000s had already had occupational education in nursing: i.e., before continuing their studies in higher education they had been working as nurses and wanted to develop further in nursing. In contrast, the nursing students of the 1990s started their nursing education straight after their secondary education (Table 3).
The changes in nursing students’ approaches to learning nursing in the 1990s and in the 2000s
In the questionnaire, the Likert scale offered choices between 1 (agree) and 5 (disagree). The smaller the mean scores, the more the respondents agreed with the statements. The extent to which the nursing students revealed different approaches to learning nursing varied in the mid-1990s and mid- 2000s (Table 4).
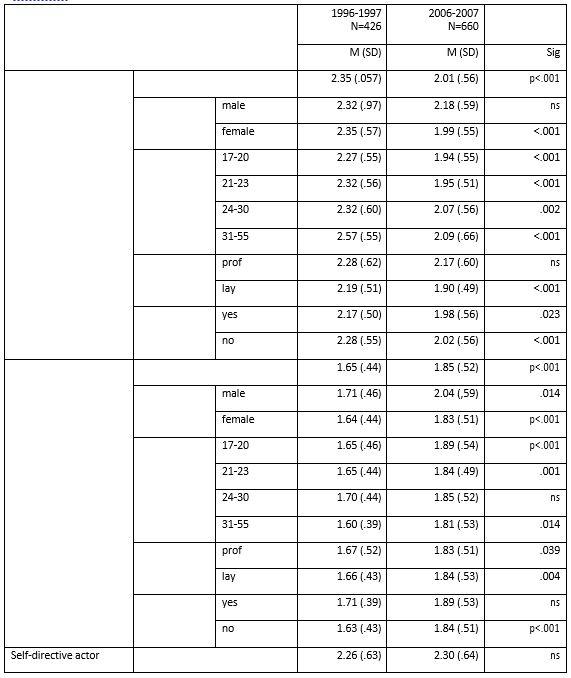
The results show that features of assisting actor were more common among the nursing students in
the mid-2000s than in the mid-1990s. The change was statistically significant (Table 4). On the other hand, the nursing students of the 1990s expressed fewer features of the co-operational actor than did those students who studied in the 2000s. However, there was no change concerning the features of the self-directive actors between the students of the 1990s and those of the 2000s (Table 4).
Connections between background variables and nursing students’ approaches to learning nursing
The results suggest that some of the background variables explain the variation among the nursing students of the different decades. The results show that the female students of the mid-2000s, in general, expressed more features of the assisting orientation to learning nursing than did those studying in the mid-1990s. On the other hand, there was no significant difference among the male students of these decades. There was a clear trend of more students in the age groups 17-20 and 21- 23 years expressing features of the assisting approach (p<.001). The nursing students who had had earlier lay experience in the field of nursing and who had studied in the mid-2000s, expressed fewer features of the assisting actor (p<.001) than did students who had studied in the mid-1990s (Table 4).
Neither the age group, sex, nor earlier professional experience in the field of nursing explained the change in nursing students’ self-directive learning approach. The only exception is the youngest age group: students between 17 and 20 years of age were significantly more oriented to self- directedness than the older students. The students of the mid-1990s who had had earlier lay experience in the field of nursing to some extent revealed more features of self-directive learning approach than did students who had studied in the mid-2000s (p=.045) (Table 4).
The background variables explained some of the changes concerning the co-operative approach to learning nursing between the students of the mid-1990s and those of the mid-2000s. Sex explained some of this change in the mid-2000s. The trend was for the expression of fewer features of the co- operational approach to learning nursing in the cohort of the mid-2000s. The difference was statistically significant in both sex groups. Moreover, the age (17-23 and 31-55 years) explained the change in demonstrating fewer features of the co-operative approach to learning nursing when coming to the mid-2000s. The students of the mid-1990s and those who had previous lay experience in the field of nursing expressed more features of co-operational actors than did the students who had studied in the mid-2000s (p=.001). Moreover, the students of the 1990s who intended to change fields in the future showed more features of co-operational actors than did those of the 2000s. The difference was statistically significant (p<.001). Among the nursing students who did not express such intentions, the trend was the same (p<.032) (Table 4).
Discussion
The aim of the study was to describe how the learning approach of nursing students in Finland has changed since 1990’s. The results suggest that the features of the assisting approach to learning nursing among nursing students were on the increase between the mid-1990s and the mid-2000s. The assisting actor approach means that the needs the teacher’s and supervisor’s support, and the encouragement of peers. However, to some extent she hesitates to take personal responsibility in patient care. This is surprising because the learning methods used nowadays are intended to promote self-directiveness among nursing students (Blake 2005; Williams & Jordan 2007; Levett- Jones 2005). However, some students are able to manage their learning process better, whereas others need more supervision (Levett-Jones 2005). According to these results, the number of features of self-directiveness has not changed among these student groups.
The nursing students of the 2000s expressed fewer features of co-operational actors than did those of the 1990s. The co-operational actor approach includes testing knowledge, ideas and practices together with peers and a multi-professional team and emphasises learning as a shared experience. The decrease of these features may be the result of the use of learning methods that support the students’ self-directive learning and individual learning processes. However, nurses have to work as full members of interdisciplinary teams in social and health care. In fact, there are some studies that support the development of interdisciplinary learning in the field of health care (Jacobsen et al.
2009; Steiner et al. 2008). In nursing education in the future, it could be valuable to pay more attention to the development of nursing students into responsible actors in multi-professional health care teams.
There are many measurement tools that can be used to analyse and evaluate the learning styles of students, and they have been used in nursing studies, too (Fountain & Alfred 2009). There are also instruments developed to measure the nurse-patient relationship from patients’ perspective (Suikkala et al. 2009) and to assess the competence of the nurses (Dellai et al. 2009).The measurement tool used in this study was specifically developed for nursing and with nursing teachers and students. As a limitation, the subscales in the measurement tool were short. In fact, it would be useful to develop more valid statements into the subscales. However, based on the results of this study, it is possible to make suggestions regarding suitable learning methods for individual nursing students. We believe that this kind of measurement tool has a place both in students’ peer and self-evaluation, and also in the discussions between supervisors and students when planning learning methods in nursing education.
Conclusions
It is worrying that there are still students in higher education in nursing who are willing to assume an assistant’s role in the field of health care. In the light of this result, it is important to develop teaching and learning methods which are based on the idea of shared learning and improve the students’ self-confidence and development towards expertise in nursing. Moreover, more attention needs to be devoted to learning how to work as a responsible member of a multi-professional team. This should be an important focus in nursing education in the future.
This was the first time that this measurement tool has been used to measure nursing students’ learning approaches in nursing. The measurement tool worked successfully when studying the changes in students’ learning approach in nursing between the 1990s and the 2000s. Furthermore, it could be useful when choosing and developing learning and teaching methods in nursing education in the international scene of higher education. While project-based nursing education, such as learning by developing (Kallioinen 2011) has been established and developed in universities of applied sciences, it would be interesting to study the learning approaches of the students of 2010s.
Acknowledgements
The authors thank Vivian Michael Paganuzzi, University of Eastern Finland, for his suggestions regarding the language and style of this paper. We are also very grateful to the nurse teachers who have helped us to collect the data, and to the nursing students who participated in our study.
Author
Liisa Vanhanen-Nuutinen, RN, MNSc, PhD, Research Manager, School of Vocational Teacher Education, HAAGA-HELIA University of Applied Sciences, Finland
Sirpa Janhonen, RN, MA, PhD, Professor (emerita), Institute for Health Sciences, Faculty of Medicine, University of Oulu, Finland
Maija Maunu, RN, MNSc, Lecturer, Degree Program in Nursing, School of Health and Social Care, Oulu University of Applied Sciences, Finland
Helena Laukkala, M.A., Lecturer,Department of Research Methodology, University of Lapland, Finland
[vc_tta_accordion active_section=”0″ no_fill=”true” el_class=”lahteet”][vc_tta_section title=”References” tab_id=”1458134585005-b3f22396-5506″]
Abel, W. M. (2006) Evaluating of Concept Mapping in an Associate Degree Nursing Program. Journal of Nursing Education, 45(9), 356-364.
Ahola, S. (2006) From ’Different but Equal’ to ’Equal but Different’: Finnish AMKs in the Bologna Process. Higher Education Policy (2006) 19, 173–186.
Apodaca, P. & Grad, H. (2005) The dimensionality of student ratings of teaching: integration of uni- and multidimensional models. Studies in Higher Education , 30(6), 723-748.
Ausubel, D. P. (1978) Educational psychology: A cognitive view. New York: Holt Rinehart and Winston.
Badeau, K.A. (2010) Problem-Based Learning. An Educational Method for Nurses in Clinical Practice.
Journal for Nurses in Staff Development 26(6), 244-249.
Bahcecik, N & Alpar, S. E. (2009) Nursing education in Turkey: From past to present. Nurse Education Today, 29(7), 698-703.
Bashook, P. G., Gelula, M. H., Joshi, M. & Sandlow, L. J. (2008) Impact of students’ reflective e-portfolio on medical student advisors. Teaching & Learning in Medicine, 20(1), 26-30.
Blake, T. K. (2005) Journaling: an active learning technique. International Journal of Nursing Education Scholarship 2(1), Article 7.
Carmines, E. G. & Zeller, R.A. (1979) Reliability and validity assessment. Beverly Hills, California: SAGE.
Davies, R. (2008) The Bologna process: The quiet revolution in nursing higher education. Nurse Education Today, 28(8), 935-942.
Dellai, M., Mortari, L. & Meretoja, R. (2009) Self-assessment of nursing competencies – validation of the Finnish NCS instrument with Italian nurses. Scandinavian Journal of Caring Science, 23(4), 783- 791.
Engeström, Y. (2001) Expansive learning at work: towards an activity-theoretical reconceptualization.
Journal of Education and Work 14(1), 133-156.
Finnish Ministry of Culture and Education, online statistics 14 April 2011.
Fountain, R. & Alfred, D. (2009) Student satisfaction with high-Fidelity Simulation: Does it correlate with learning styles. Nursing Education Research, 30(2), 96-98.
Gillespie, M. (2005) Student teacher connection: a place of possibility. Journal of Advanced Nursing. 52(2), 211-219.
Greenwood, J. (1998) The role of reflection in single and double loop learning. Journal of Advanced Nursing, 27(5) 1948-53.
Guile, D. & Griffiths, T. (2001) Learning through work experience. Journal of Education and Work 14(1), 113-131.
Hay, D. B. (2008) Developing dialogical concept mapping as e-learning technology. British Journal of Educational Technology 39(6), 1057-1060.
Hsu, L. L. (2004) Developing concept maps from problem-based learning scenario discussions.
Journal of Advanced Nursing 48(5), 510-518.
Jacobsen, F., Fink, A.M., Marcussen, V. Larsen K., and Hansen T. B. (2009)
Interprofessional undergraduate clinical learning: Results from a three year project in a Danish Interprofessional Training Unit. Journal of Interprofessional Care 23(1), 30-40.
Kallioinen, O. (2011) Transformative Teaching and Learning by Developing. Journal of Career and Technical Education 26(2).
Khomeiran, R. T, & Deans, C. (2007) Nursing education in Iran: Past, present, and future. Nurse Education Today 27(7), 708-714.
Knowles, M. (1980) The modern practice of adult education: from pedagogy to andragogy. Chicago: Follet.
Kuuppelonmäki, M., &Tuomi, J. (2005) Finnish nurses’ attitudes towards nursing research and related factors. International Journal of Nursing Studies, 42, 187-196.
Kyrkjebo, J. M., Mekki., T. E. & Hanestad, B. R. (2002) Issues and innovations in nursing education. Short report: Nursing education in Norway. Journal of Advanced Nursing, 38(3), 296-302.
Lave, J. & Wenger, E. (1991) Situated learning: Legitimate peripheral participation. New York: Cambridge University Press.
Levett-Jones, T.L. (2005) Self-directed learning: implications and limitations for undergraduate nursing education. Nurse Education Today, 25(5), 363-368.
Marton, F. & Säljö, R. (1976) On qualitative differences in learning – 1: outcome and process. British Journal of Educational Psychology 46, 4-11.
Nunnally, J. C. & Bernstein, I. H. (1994) Psychometric Theory. Third Edition. New York: McGraw-Hill. Perälä, M.-L. & Ponkala, O. (1999) Tietoa ja taitoa terveysalalle – terveysalan korkeakoulutuksen arviointi. Korkeakoulujen arviointineuvoston julkaisuja no 8. Helsinki, Edita.
Ponkala, O. (toim.) (2001) Terveysalan korkeakoulutuksen arvioinnin seuranta. Korkeakoulujen arviointineuvoston julkaisuja no 11. Helsinki, Edita.
Pratt, J. (1997) The Polytechnic Experiment: 1965-1992. The Society for Research into Higher Education. Bristol: Open University Press.
Romyn, D. (2001) Disavowal of the the behavioristic paradigm in nursing education: What makes it so difficult to unseat? Advances in Nursing Science, 23(3), 1-10.
Roxburgh, M., Watson, R., Holland, K., Johnson, M., Lauder, W., Topping, K. (2008) A review of curriculum evaluation in United Kingdom nursing esucation. Nurse Education Today 28, 881-889. Statute (2003) Statute concerning the universities of applied sciences 351/2003 (Finland).
Statute (2003) Statute concerning degrees in universities of applied sciences 352/2003 (Finland). Steiner, J. L., Ponce, A. N., Styron, T., Aklin, E. E. & Wexler, B. E. (2008) Teaching an interdisciplinary approach to the treatment of chronic mental illness: challenges and rewards. Academic Psychiatry 32(3), 255-258.
Suikkala, A., Leino-Kilpi, H. & Katajisto, J. (2009) Factors related to the nursing student-patient relationship: the patients’ perspective. Scandinavian Journal of Caring Sciences, 23(4), 625-634. Svavarsdottir, E. K. (2008) Excellence in Nursing. A Model for Implementing Family Systems Nursing in Nursing Practice at the Institutional Level in Iceland. Journal of Family Nursing, 14(4), 456-468.
Turale, S., Ito, M. & Nakao, F. (2008) (Quest Editorial) Issues and challenges in nursing and nursing education in Japan. Nurse Education in Practice, 8(1) 1-4.
Tynjälä, P. (2008) Perspectives into learning at the workplace. Educational Research Review, 3(2), 130-154.
Williams, B. (2004) Self direction in a problem based learning. Nurse Education Today 24(4), 277-285. Williams, M. & Jordan, K. (2007) The nursing professional portfolio: a pathway to career development. Journal of Nurses in Staff Development, 23(3), 125-131.
[/vc_tta_section][/vc_tta_accordion]